
When Health Coverage Isn’t Care
Rebuilding Healthcare Through Market Discipline, Not More Government

Hello friends,
A recent Wall Street Journal investigation into Medicaid’s “ghost networks” exposes a hard truth that policymakers refuse to confront: government is very good at expanding healthcare coverage, but consistently fails at delivering health care.
Millions of Americans with taxpayer-subsidized Medicaid receive insurance cards listing dozens of “in-network” doctors. But when they try to book an appointment, they face waits, disconnected phone numbers, inaccurate directories, or specialists who haven’t treated a Medicaid patient in years.
This isn’t a fluke. It’s the predictable outcome of a healthcare system built on distorted incentives, rigid price controls, and decades of federal policy that disconnect patients from prices, providers, and responsibility.
As Washington debates shifting ACA tax credits, the real crisis lies much deeper. What America needs is a structural shift toward personal responsibility, transparent market prices, and competitive markets—the principles behind the Empower Patients Initiative.

A 1940s Tax Policy Still Distorts Healthcare Today
America’s employer-based insurance system didn’t emerge because it worked better. It arose as a workaround to World War II wage and price controls and was later cemented by the federal tax code. That temporary fix has grown into one of the largest tax expenditures in the federal budget—roughly $27,000 per family in untaxed compensation.
As outlined in the Empower Patients initiative, this exclusion:
hides the actual cost of insurance,
reduces wage transparency,
traps workers in employer plans,
inflates premiums by subsidizing overconsumption, and
shifts power away from patients and toward employers and insurers.
Any reform that leaves this exclusion untouched cannot fix healthcare’s incentive problem. Redirecting subsidies—no matter how cleverly designed—still props up a system that treats insurers and government agencies as the primary decision-makers rather than individuals.
The real free-market correction is straightforward: end the current tax exclusion and redirect some or all of it into portable, no-limit Health Savings Accounts (HSAs). This would immediately strengthen price discipline, force insurers to compete directly for consumers, and restore patient autonomy.
Why Medicaid Fails: Misaligned Incentives and Rationed Access
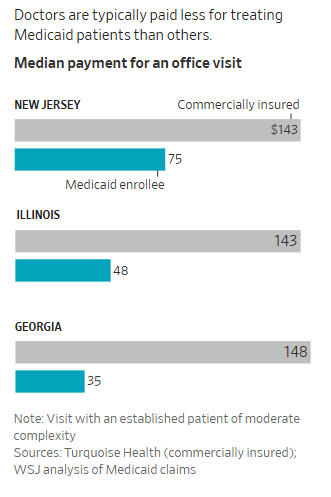
The WSJ findings reinforce what health-policy scholars have long understood: Medicaid’s incentive structure guarantees limited access. Reimbursement rates far below market levels discourage specialist participation.
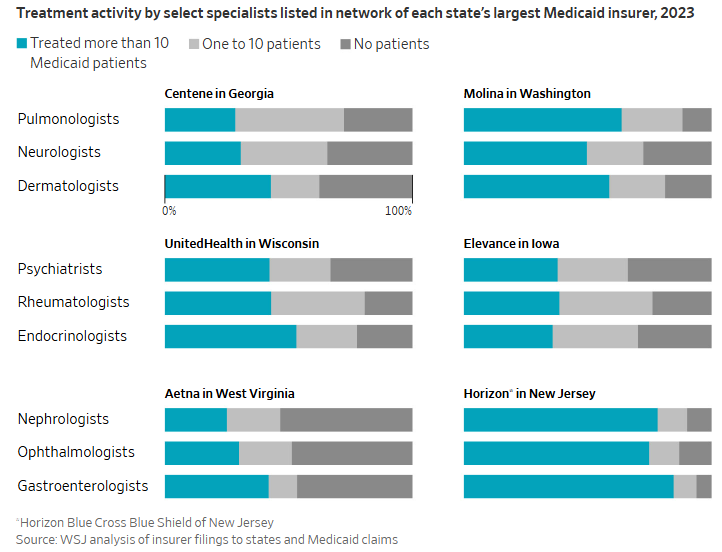
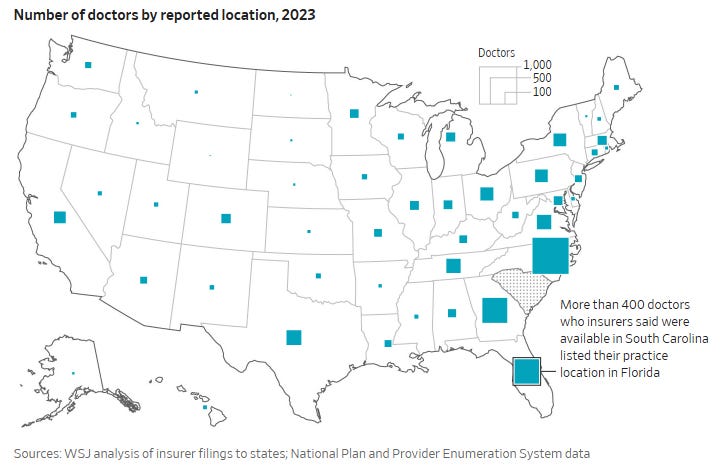
States rely on insurers’ self-reported provider directories, creating widespread “ghost networks.” Patients wait months or years for specialty care, endure canceled appointments, and navigate directories filled with outdated or inactive providers.
That’s not compassion. That’s rationing by delay.
A more humane approach—central to Empower Patients—is for the federal government to give block grants to states so they can experiment with options like allowing Medicaid enrollees to have HSAs that roll over, paired with access to catastrophic private insurance. This model:
empowers low-income families to choose their providers,
expands access by integrating them into competitive markets,
encourages preventive care and responsible spending, and
reduces long-run costs by restoring price signals.
Redirecting ACA Credits Doesn’t Fix the Core Problem
Proposals to send ACA subsidies directly to individuals instead of insurers are a marginal improvement—but they leave the core structure intact. They subsidize comprehensive, high-premium plans shaped by federal mandates. They insulate consumers from prices. And they entrench third-party payment systems that drive costs higher.
Real reform—consistent with the Empower Patients initiative—requires:
ending the employer tax exclusion,
allowing no-limit HSAs to everyone, and
deregulating provider supply.
That’s how you shift healthcare from bureaucracy to consumer sovereignty.
This Also Helps Solve Washington’s Spending Crisis
Healthcare is the dominant driver of America’s long-term fiscal imbalance. Medicaid, Medicare, ACA subsidies, and healthcare tax expenditures account for trillions in unfunded liabilities.
Ending the employer exclusion and realigning incentives through HSAs would:
reduce long-run federal tax expenditures,
lower premiums by increasing price sensitivity,
reduce reliance on federal subsidies,
encourage preventive and cost-effective care, and
naturally slow the growth of federal health spending.
This is one of the rare reforms that addresses both the access crisis and the spending crisis simultaneously.
The Path Forward
A functional, humane, and economically sustainable healthcare system must rest on three principles:
Universal, portable, no-limit HSAs funded by redirecting tax exclusions directly to individuals
Block grants to states for Medicaid HSAs with rollover, integrating low-income families into the same competitive marketplace
A supply-expanding, price-transparent market driven by competition, innovation, and voluntary exchange
Coverage is a statistic reported to government agencies. Care is what people actually need. And only a market-driven system—rooted in personal choice, transparent prices, and direct accountability—can reliably deliver it.
Thanks for reading. If this resonated, please share it, subscribe, and help push the healthcare debate back toward solutions that actually work.
More soon,
Vance Ginn, Ph.D.
—
For more research, policy frameworks, and commentary on restoring patient-centered healthcare, visit vanceginn.com.